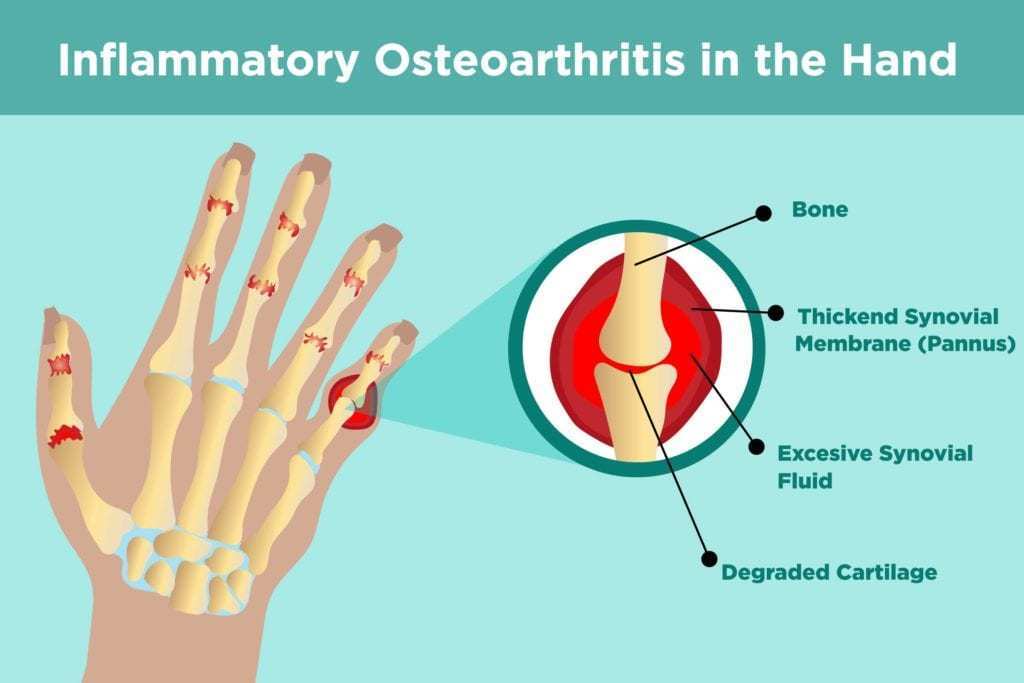
Osteoarthritis (OA) in the hand is the most common musculoskeletal disorder in people over 65 years old. It happens 2.6 times more likely to happen with women as well. It’s symptomatic in about 10-25% of the population who has the disorder already. It’s also thought to have a possible genetic link, so your mom and mom’s mom might have OA in their hands as well.
Getting technical with it, Osteoarthritis is when the hyaline cartilage in between joints, which acts as a shock absorber, starts to degrade. That’s when people start to feel that “bone-on-bone” grinding. It’s uncomfortable and really takes a toll on everyday life.
So what causes it? It’s still a bit unclear, but from what we know, repetitive usage (this one isn’t as black and white as far as a cause), previously injured joints, and lax, deformed, or misaligned joints. This tends to be more for those who are doing hard labor (factories, construction, etc.).
It should also be noted since this is a chiropractic blog that “cracking” your knuckles does NOT lead to OA in the hands no matter how long or how often you do it. We wouldn’t be the most effective profession if mobilizing/“cracking” joints caused OA, now would we?
Moving on. What makes OA worse? Obesity. Obesity basically causes a bunch of inflammation in the body which makes just about everything a lot harder. That’s my technical way of putting it. Studies have shown that while it’s not a direct mechanical cause, the biochemical pathways that lead to inflammation brought on from obesity doesn’t help with OA at all.
What can we do to help? I’m glad you asked. Our number 1 goal is to always get you out of pain because that leads to better function and that’s what we are all about here. While we reduce pain, we want to improve strength and range of motion. All sounds dandy right? I think so too. We will do this by light adjustments, exercises, soft tissue modalities (like Graston), splints, and ADL advice. We might also recommend more passive care modalities, like paraffin baths.
Acupuncture and low level lasers are still on the fence about if they really help with OA, but it’s still something we can absolutely look into if need be. The same goes for chondroitin sulfate and glucosamine sulfate supplements, as well as oral NSAIDS. Topical NSAIDS have been shown to be a safer alternative. Injections are said to help with pain management and in worst cases, a surgical joint replacement is considered.
So that’s my spiel on osteoarthritis in the hands! If you all have any questions, comments, or concerns, feel free to email us at [email protected]. If you want to schedule an appointment or see more information about us head to wurthchiro.com!
References:
1. Loughlin J. The genetic epidemiology of human primary osteoarthritis: current status. Expert reviews in molecular medicine. 2005 May;7(9):1-2.
2. Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. The Lancet. 2005 Mar 12;365(9463):965-73.
3. Anderson JJ, Felson DT. Factors associated with osteoarthritis of the knee in the first national Health and Nutrition Examination Survey (HANES I) evidence for an association with overweight, race, and physical demands of work. American journal of epidemiology. 1988 Jul 1;128(1):179-89.
4. Yusuf E, Nelissen RG, Ioan-Facsinay A, Stojanovic-Susulic V, DeGroot J, van Osch G, Middeldorp S, Huizinga TW, Kloppenburg M. Association between weight or body mass index and hand osteoarthritis: a systematic review. Annals of the rheumatic diseases. 2010 Apr 1;69(4):761-5.
5. Villafañe JH, Valdes K. Combined thumb abduction and index finger extension strength: a comparison of older adults with and without thumb carpometacarpal osteoarthritis. Journal of manipulative and physiological therapeutics. 2013 May 1;36(4):238-44.
6. Schultz RJ, Krishnamurthy S, Thelmo W, Rodriguez JE, Harvey G. Effects of varying intensities of laser energy on articular cartilage: a preliminary study. Lasers in surgery and medicine. 1985;5(6):577-88.
7. Hegeds B, Viharos L, Gervain M, Gálfi M. The effect of low-level laser in knee osteoarthritis: a double-blind, randomized, placebo-controlled trial. Photomedicine and laser surgery. 2009 Aug 1;27(4):577-84.
8. Ye L, Kalichman L, Spittle A, Dobson F, Bennell K. Effects of rehabilitative interventions on pain, function and physical impairments in people with hand osteoarthritis: a systematic review. Arthritis research & therapy. 2011 Feb;13(1):R28.